
Review
GLP-1 receptor agonist adjunct therapy stabilises Ramadan dysglycaemia in insulin-treated diabetes: a CGM-based study
Tanveer Ashraf a,*,1 , Nader Lessan b
a Clinical Research Fellow, Imperial College London Diabetes and Endocrine Centre (ICLDEC), Abu Dhabi, United Arab Emirates
b Consultant Endocrinologist and Diabetologist, Clinical Lead in Research, Imperial College London Diabetes and Endocrine Centre (ICLDEC), Visiting Reader, Imperial College London, UK
ARTICLE INFO
Edited by Dr G Liu
Keywords:
Ramadan fasting
Type 2 diabetes
Type 1 diabetes
Continuous glucose monitoring GLP-1 receptor agonist
GLP-1/GIP dual agonist Tirzepatide
Semaglutide
Post-iftar hyperglycaemia Time in Range
Highlights
- Dual GLP-1R/GIPR agonism mitigates endothelial dysfunction and suppresses inflammatory pathways driving AAA progression.
ABSTRACT
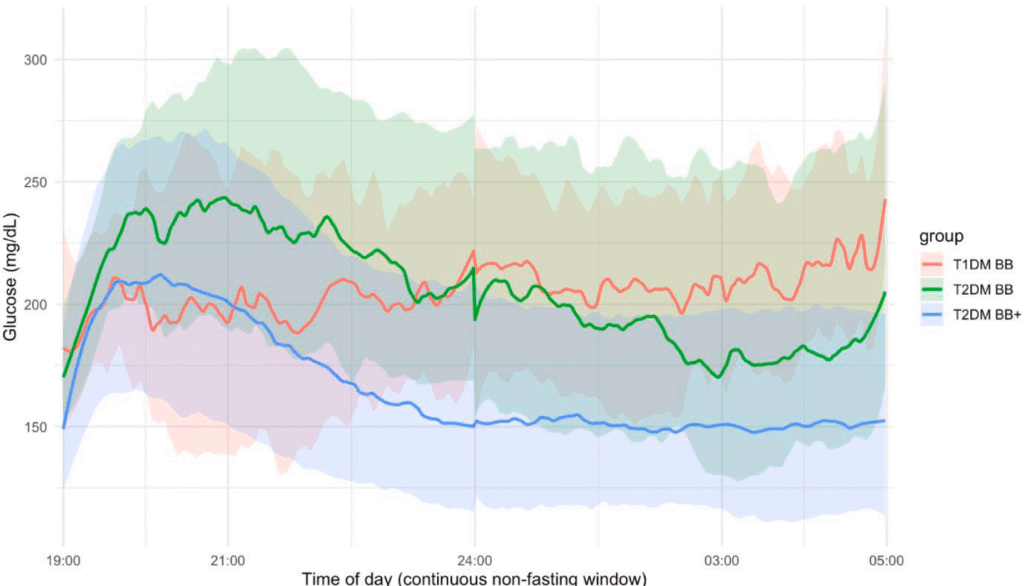
Background: Patients with type 1 and insulin-treated type 2 diabetes are at higher risk of hypo- and hyper- glycaemia during Ramadan fasting. The role of incretin-based add-on therapy (GLP-1 receptor agonist sem- aglutide and the GLP-1/GIP dual agonist tirzepatide) in attenuating Ramadan dysglycaemia in insulin-treated type 2 diabetes has not been characterised using continuous glucose monitoring. Emerging evidence indicates that exaggerated post-iftar hyperglycaemia, drives Ramadan dysglycaemia in insulin-treated individuals. Aims: To use continuous glucose monitoring (CGM) to characterise glycaemic control in patients with type 1 and type 2 diabetes on intensive insulin during Ramadan fasting, and to evaluate the role of add-on semaglutide or tirzepatide in attenuating post-iftar hyperglycaemia.
Methods: Adults with type 1 or type 2 diabetes using FreeStyle Libre CGM who completed ≥ 14 full fasting days during Ramadan 2025 were included. Of 140 participants screened pre-Ramadan, 54 met all inclusion criteria and were analysed: type 2 diabetes on basal–bolus insulin alone (BB, n = 18), type 2 diabetes on basal–bolus plus tirzepatide or semaglutide (BB+, n = 18) – matched 1:1 by age, baseline HbA1c and BMI – and type 1 diabetes on basal–bolus insulin (T1DM, n = 18). CGM metrics were collected over 28 days pre-Ramadan (1–28 February 2025) and 29 days during Ramadan (1–29 March 2025) and compared within and between groups, and across fasting versus non-fasting windows.
Results: Dysglycaemia was driven predominantly by the post-iftar period. BB participants showed marked deterioration during non-fasting hours. Adjunctive therapy attenuated this effect: time in range 74.4 % vs 36.8 % (p = 0.007), glucose management indicator 6.9 % vs 8.3 % (p = 0.004), and > 2-fold (≈61 %) reduction in incremental post-iftar area under the curve (102,014 vs 260,578 mg/dL⋅min over the 4-h post-iftar window). Conclusion: In matched insulin-treated type 2 diabetes cohorts, add-on semaglutide or tirzepatide stabilised Ramadan glycaemia and reduced post-iftar hyperglycaemia without increasing hypoglycaemia, and was well tolerated with no treatment discontinuations during Ramadan.
Article
In matched insulin-treated type 2 diabetes cohorts, add-on semaglutide or tirzepatide stabilised Ramadan glycaemia and reduced post-iftar hyperglycaemia without increasing hypoglycaemia, and was well tolerated with no treatment discontinuations during Ramadan.
These results provide actionable guidance for clinicians and support the integration of GLP- 1RA co-therapy into personalised Ramadan care pathways for in- dividuals requiring intensive insulin therapy.
Available online July 14, 2026
2308-8567/© 2026 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY license (http://creativecommons.org/licenses/by/4.0/).